Medical emergency response services provide assistance to events of illness or injury that require urgent attention. In the basic medical emergency response service, an ambulance is required to provide treatment and transportation. The efficiency of an emergency service has an effect over the wellbeing of the society since timely medical attention can reduce suffering, mortality or disability risks. Therefore, is essential that the institution -or government entity- that provide the emergency service define an acceptable emergency response time.

The response time is measured as the time starting with the end of the emergency call and ends when the ambulance gets to the call site. Preparedness is measured per zone by checking that at least one ambulance is able to aid a call under an acceptable response time. (Andersson, Petersson, and Varbrand 2004)(Shuib and Zaharudin 2011) (Zaharudin et al. 2012) By comparing this suitable response time with their actual response time and preparedness, the provider is able to measure an instance of the emergency service quality. (Hafiz et al 2013) (Zaharudin et al. 2012)
According to international standards, an acceptable reference response time is of 15 minutes. This time can differ as the emergency service provider considers it necessary. For example, in United States the response time is of 10 minutes for cities and 30 minutes for rural areas for 95% of the calls; but in Montreal, QC, Canada it is 7 minutes for 90% of the calls. This can vary as well depending of the urgency level of the call; for instance, Stockholm considers a response time of 10 minutes for 75% of potentially mortal calls and of 20 minutes for 99% of non-urgent calls. (Andersson, Petersson, and Värbrand 2007) (Gendreau, Laporte, and Semet 1997) (Hafiz et al. 2012) (Sanchez 2012)
In order to comply with the expected efficiency levels of emergency response services, multiple ambulance location models have evolved over the past 30 years. Ambulance allocation models are meant to assure maximal coverage of service under an acceptable response time while some considers a limited number of ambulances or other restrictions. Moreover, the advances in the available technologies were useful in order to consider more factors and reduce calculation times. These mathematical models are classified mainly in three categories: deterministic, probabilistic and dynamic models.
Deterministic models
Deterministic models were the first to be adapted to the ambulance location and are used currently during the initial planning phase since they are simple and use basic information of the problem. Some of these models are:
- Location Set Covering Model (LSCM) is used to determine the number of ambulances needed to cover the demand.
- Maximal Covering Location Problem (MCLP) is used to maximize coverage of demand using a limited number of ambulances. The next figure shows a graphical representation of this model. The next figure shows the demand and optimal location of ambulances which guarantees the maximum possible coverage with the available ambulances.
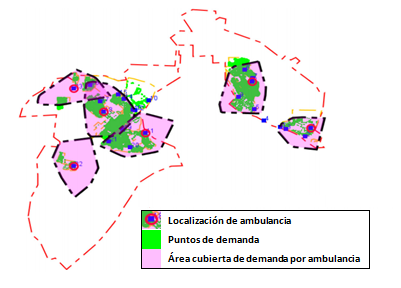
MCLP MODEL BASED IN DEMAND AND POSSIBLE LOCATIONS FOR AMBULANCES. (HAFIZ ET AL. 2012)
Probabilistic models
Probabilistic models are based on deterministic models but they consider unknown circumstances, such as the probability of an ambulance being busy or demand variation over time. Some of these models are:
- Maximum Expected Covering Location Problem (MEXCLP) is used to maximize coverage considering a limited number of ambulances and the probability of a busy ambulance.
- Maximum Expected Covering Location Problem with Time Variation (TIMEXCLP) is used to maximize coverage of demand considering the probability of a busy ambulance and variations in travel speed during the day.
- Dynamic models are based in the previously descripted models but additionally it is recalculated every time an ambulance is needed or in a period of time. For instance, the
- Double Standard Redeployment Problem (DSRP) complements probabilistic models with a fast taboo search heuristic which allows running the algorithm non-stop until the best solution is obtained.
Localization models
During the localization models’ implementation, it is highly recommended to consider external components such as traffic demand and costs of providing the service to ensure success and reliability of the results. (Brotcorne, Laporte, and Semet 2003)(Shiah, Hung, and Chen, 2009)
The usage of such location and optimization models has provided savings and improvements over response times. For instance, in Austin, Texas during 1984 a reduction in average response time, savings of $3.4 million USD in construction costs and $1.2 million in operative costs were reported by using the deterministic model MCLP. (Brotcorne, Laporte, and Semet 2003) Louisville, Kentucky reported an increase in coverage and a reduction of 36% of their average response time using a probabilistic model. (Rajagopalan, Saydam, and Xiao 2005) A dynamic model based in DSRP has been in development since 2008 and has resulted in 75% of coverage with a response time of 8.49 minutes, according to preliminary analysis. (Céspedes, Amaya, and Velasco 2008)
In conclusion, using analytics to improve emergency services is necessary not only to guarantee good service, but also to to lower the costs of the service and to fulfill standards. (Brotcorne, Laporte, and Semet 2003) (Sanchez 2012) TIS Consulting Group has considered these studies to support medical institutions and improve their level of service. With these implementations, savings are then available for other improvements within the institution, while guaranteeing efficiency on its mobile health care service.
References:
Andersson, Tobias, Sverker Petersson, and Peter Varbrand. 2004. “Calculating the Preparedness for an Efficient Ambulance Health Care.” Intelligent Transportation Systems, 2004. Proceedings. The 7th International IEEE Conference On (October 6): 785,790.
Andersson, Tobias, Sverker Petersson, and Peter Värbrand. 2007. “Decision Support for Efficient Ambulance Logistics.”Linköping University. http://webstaff.itn.liu.se/~toban/Andersson2007.pdf.
Brotcorne, Luce, Gilbert Laporte, and Frédéric Semet. 2003. “Ambulance Location and Relocation Models.” Elsevier Science B. V. European Journal of Operational Research: 451–463.
CAPUFE. 2008. “Normatividad Para La Operación de Los Servicios Médicos.” Caminos y Puentes Federales de Ingresos y Servicios Conexos, México. January 22. http://www.capufe.gob.mx/normateca/normas/164_Normat_para_la_Opera_de_los_Servicios_Med_22012008/NormaServiciosMedicos.pdf.
Céspedes, S. M., C. A. Amaya, and N. M. Velasco. 2008. “Localización y Relocalización de Ambulancias Del Centro Regulador de Urgencias y Emergencias de Bogotá.” Universidad de Los Andes. December. http://dspace.uniandes.edu.co/xmlui/bitstream/handle/1992/1121/H%202008%2023.pdf?sequence=1.
Gendreau, Michel, Gilbert Laporte, and Frédéric Semet. 1997. “Solving an Ambulance Location Model by Tabu Search.”Location Science 5 (2) (August): 75–88.
Hafiz, M., C. Siong, W. A. Lutfi, W. M. Hatta, and L. Chai. 2012. “Application of OpenStreetMap Data in Ambulance Location Problem.” IEEEXplore. http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=6274362.
Hafiz, M., C. Siong, W. A. Lutfi, T. Loong, and S. Siang. 2013. “Simulation of Emergency Medical Services Delivery Performance Based on Real Map.” International Journal of Engineering and Technology 5 (3) (June): 2620–2627.
Rajagopalan, H. K., C. Saydam, and J. Xiao. 2005. “A Multiperiod Expected Covering Location Model for Dynamic Redeployment of Ambulances.” Advanced OR and AI Methods in Transportation (December 19). http://www.iasi.cnr.it/ewgt/16conference/ID63.pdf.
Sanchez, Ana R. 2012. “Cruz Roja Necesita Apoyo Para Ambulancias.” El Imparcial, November 3. http://www.elimparcial.com/EdicionEnLinea/Notas/Noticias/11032012/578343.aspx.
Shiah, Dah-Ming, Chin-Tun Hung, and Shu-Wen Chen,. 2009. “Multi-Capacities Ambulance Location Model.” Testbeds and Research Infrastructures for the Development of Networks & Communities and Workshops, 2009. TridentCom 2009. 5th International Conference On (April): 1,6–8.
Shuib, A., and Z. A. Zaharudin. 2011. “TAZ_OPT: A Goal Programming Model for Ambulance Location and Allocation.” IEEE Xplore. http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=6163878.
Zaharudin, Z. A., N. A. Nordin, H. M. Tahir, C.W.R.A.C. Kamal, N.H.A. Ghani, and N.H.A. Halim. 2012. “An Application of MEXCLP Model: A Case Study for Mobile Ambulance Location.” Humanities, Science and Engineering (CHUSER), 2012 IEEE Colloquium On (December): 539,543,3–4.